Theoretical frameworks & definitions
Explore the foundational concepts that underpin the ACE indicators within Electronic Health Records.
This page provides a comprehensive overview of the key theoretical frameworks used to understand the impact of ACEs on individuals and their development.
Background
Adverse childhood experiences (ACEs) are potentially traumatic, neglectful or violent experiences in childhood. Examples of ACEs range from child maltreatment and witnessing violence in the home to growing up with a parent with a mental health problem1.
The concept of adversity is not new. However, the term "ACEs" was first introduced by a groundbreaking study published in 1998 by the Centers for Disease Control and Prevention (CDC) and the Kaiser Permanente health care organisation in California, USA2. Led by co-principal investigators Dr Vincent Felitti and Dr Robert Anda, the study originated from repeated clinical observations within an obesity treatment programme during the 1980s. As doctors gathered patient histories, they noticed that severe weight gain, smoking, and substance use were frequently linked to early abuse or household dysfunction3.
They hypothesised that for many people, severe weight gain may be the result of an unconscious coping mechanism to manage unrecognised childhood trauma2. This led to a study evaluating over 17,000 adult patients, where the researchers established a strong dose-response relationship between the number of ACEs and health problems in adults, including premature death.
The concept of ACEs helped bring together and measure a diverse set of preventable adverse childhood experiences that can lead to considerable long-term health problems, and can substantially pressure families, health and social care systems1.
The Original Ten ACEs
The initial ACEs predominately referred to domains of adversity in the home environment. They are typically categorised into the following main groups:
Child maltreatment
- Psychological abuse
- Physical abuse
- Sexual abuse
- Physical neglect*
- Emotional neglect*
Household dysfunction
- Substance abuse
- Mental illness
- Intimate partner violence†
- Criminal behaviour
- Parental separation*
Definition of ACEs
ACEs can be defined as any experience within the family environment considered to be:
- Frightening, violent, traumatic or neglectful (see WHO violence definition), with potential for immediate or longer-term harm to a child's biopsychosocial development (intentionally or unintentionally) (see UK government definition);
- Caused by a single event or through repeated exposure;
- Caused by external factors and not the child themselves, such as self-harm; and
- Amenable to health or social care intervention at a family level (i.e. excluding wider factors such as socioeconomic status, community violence, school bullying etc)*.
*Refers to the ACEs included as part of the research examining ACEs using electronic health records 1, 2, 3.
Read full inclusion criteria and rationaleTheory and frameworks
A conceptual model of ACEs: the biopsychosocial approach
The concept of ACEs is not based on a single theory. Instead, it is best understood through an integrative biopsychosocial model that combines psychological, biological, and sociological perspectives. The goal of this model is to explain why ACEs occur, how they lead to long-term health and social problems, and why their effects vary depending on the specific type or number of adversities experienced.
This model uses the socio-ecological systems theories of Bronfenbrenner (1977) and Belsky (1980) as a foundational platform. By focusing specifically on the first two ecological levels—the individual and the family environment—this approach deliberately restricts the definition of ACEs to those that are clinically measurable and intervenable at the family level, whilst acknowledging that other adversities occur in the wider community.
Across these two ecological levels, the model integrates several key frameworks to predict and understand relevant ACEs. These include attachment theory (Bowlby, 1969–1982; Ainsworth et al., 1978), the cumulative stress model (encompassing both the "allostatic load" and "ecobiodevelopmental" frameworks), and cognitive behavioural theories of emotion.
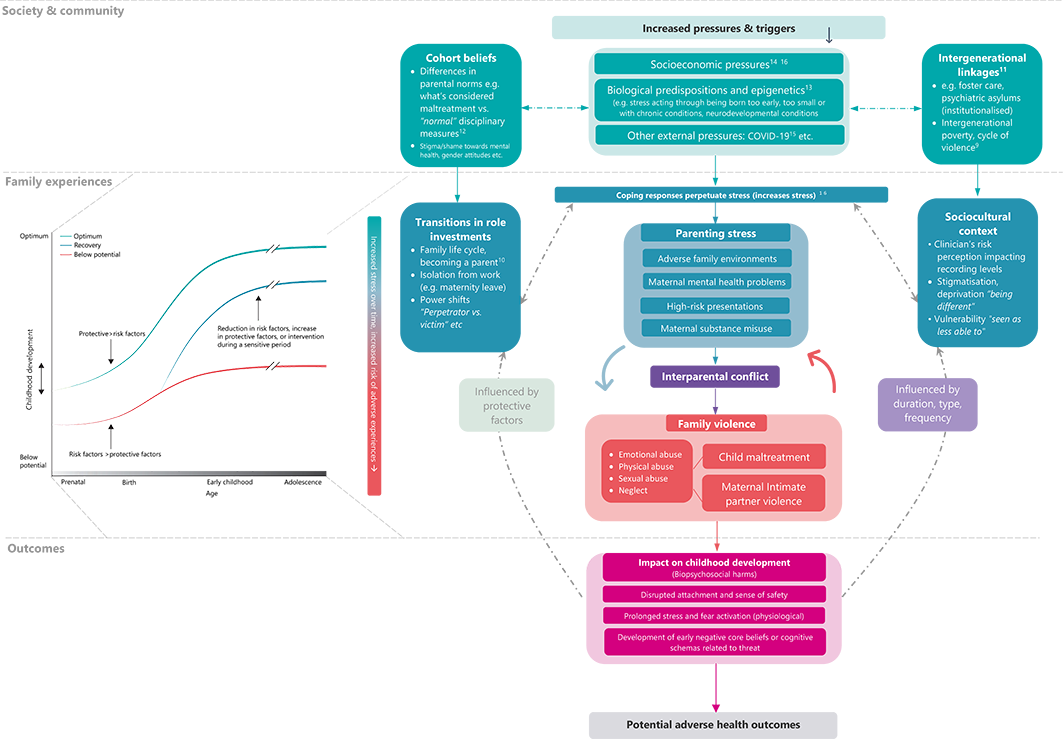
The figure does not represent an exhaustive list of potential mechanisms behind ACEs.
View Figure in High ResolutionEcological Levels & Theoretical Mechanisms
Below, we summarise different key theories and mechanisms hypothesised to play a role in the ACEs framework. It does not represent an exhaustive list.
Society & community level
Social determinants of health encompass socioeconomic conditions that shape health outcomes for individuals, families, and communities. Children with ACEs are more likely to grow up in environments where raising a family and coping with everyday challenges is harder due to:
Specific Socioeconomic Factors
- Economic instability: Living in communities with high unemployment and a lack of local family resources.
- Family deprivation (housing & food insecurity, etc.): Not having the financial means to reliably access nutritious meals, living in poor housing conditions (e.g., overcrowding, lack of heat, environmental toxins like lead), and a lack of safe spaces to play.
- Neighbourhood violence: Exposure to community violence or high crime rates is actually considered a "community-level ACE" by many modern frameworks. It directly forces the "survival strategies" mentioned later in the text.
- Healthcare and educational barriers: A systemic lack of access to preventive care, health services, or health insurance, alongside underfunded local schools and a lack of access to early childhood education.
- Geographic barriers: Parents having to travel long distances for work.
- Systemic racism and discrimination: Marginalisation based on race, ethnicity, or immigration status impacting access to resources.
- Health barriers: Family members suffering from health problems that make it difficult to maintain employment.
Individual & family level
Attachment and learning theory
Social risk factors can negatively influence a carer's availability and responsiveness to a child's needs and attachment cues. The potential impact in the early years includes:
Potential Early Years Impacts
- Insecure & disorganised attachments: It can occur when the caregiver is simultaneously the child's source of safety and their source of stress or fear, leaving the child with no coherent strategy for seeking comfort. Later on, this could result in reduced emotional validation from caregivers (e.g., failing to reinforce that "my pain matters").
- Negative internal working models: Children may develop a blueprint of relationships where they view themselves as unworthy of care and others as inherently untrustworthy.
- Poor emotion regulation: Infants rely on caregivers to soothe their nervous systems (co-regulation). When this is absent, children may be more vulnerable to difficulty regulating their body's stress responses, and more easily triggering "fight, flight, freeze".
- Observational learning: Children with a carer who is under stress and struggles to cope experience reduced healthy parental modelling. Children may also learn and adopt harmful coping mechanisms (e.g., aggression) observed in their environment.
Life-course & trauma-informed approach
This model views ACEs as a complex social phenomenon, recognising families as resilient and constantly striving to cope using available resources. The model helps by:
Life-Course Model Benefits
- Separating experience from response: The model distinguishes the adverse experience from the adverse stress response, overcoming previous limitations of reverse causality when evaluating long-term outcomes.
- Family level focus: Whilst ACEs can occur outside the home and immediate family context, in our model we consider only ACEs that were recorded at the family level as amenable to service intervention and highly relevant to Electronic Health Records (EHRs).
- Acknowledging dynamic risk, resilience, and preventing stigma: Consistent with the WHO’s Minsk Declaration, the life-course approach acknowledges that risk is not static. Instead, it depends on the continuous interaction of multiple promotive, protective, and risk factors throughout a person's life. As such, families may move in and out of states of vulnerability to ACEs over time, and most children who experience ACEs do not go on to develop long-term health problems.
Cognitive and behavioural theories
Children who grow up in dangerous, unpredictable, or highly stressful environments are more likely to perceive the world as unsafe and doubt their ability to manage challenges. To cope, children may develop cognitive survival strategies (such as anticipating threats) alongside emotional and behavioural responses (like avoidance, escape, or fighting, suppressing emotions). While these mechanisms hold short-term functional value and provide a short-term sense of safety, they can increase and maintain long-term health risks by:
Long-Term Health Risks & Coping Behaviours
- Core beliefs & cognitive biases: Children may develop a heightened focus on threats, suppress their emotions, and avoid situations they fear will cause distress (aligning with theories on emotional processing and overestimation of threat). They may also develop deeply held "core beliefs"—not only that the world is unsafe, but that they themselves are fundamentally flawed or unlovable.
- Smaller window of tolerance to stress (Heightened state of alert vs. shutting down): Survival strategies overemphasise threats, creating an alert state that is difficult to "turn off" (toxic stress), leading to a smaller window of tolerance to stress and perceived threat. Alternatively, when the nervous system is completely overwhelmed, it may default to a "shut down" state, leaving children with a drastically smaller window of tolerance to everyday stressors.
- Passive vs. active survival strategies: While some children rely on active strategies (fight, flight, freeze), others may develop learned helplessness (becoming passive) or rely on dissociation (mentally "checking out" or emotionally numbing when overwhelmed). For example, when a child grows up in an unpredictable environment where nothing they do stops the adversity, they may learn that their actions don't matter.
- A maintenance cycle of stress: Survival responses prevent opportunities for new learning and balanced cognitive appraisals (e.g., realising "I'm safe" or "I can cope").4, 5
- Social isolation: Ultimately, these difficulties and coping responses may mean a child loses friends, adult support, and misses out on opportunities to build vital social networks.
Family maintenance cycle & Intergenerational transmission: As underlying stress increases, caregivers and children have fewer resources to regulate responses (e.g., reduced executive functioning)6, increasing the risk of immediate, reactive coping strategies to escape or re-gaining control (e.g. shouting, violence, neglect). For some families, these social risk factors and coping responses are carried over across generations as children become parents themselves.
A spectrum of coping responses: Behaviours may vary as a function of the level of need to escape distress, ranging from immediate escape (e.g., substance misuse, abandonment/neglect), asserting power (e.g, violence), to stronger forms of avoidance (e.g., refusing to leave the house), which further degrades long-term social support systems.7
Adverse Childhood Experiences (ACEs) using Electronic Health Records (EHRs)
A multistage risk prediction model to determine relevance of candidate ACEs
We assessed the relevance of identified candidate ACE indicators based on their consistent risk association with a reference standard of family violence in a multistage prediction model. The reference standard (outcome) was any occurrence of child maltreatment (CM) and maternal intimate partner violence (mIPV) up to 5-years post-birth.
Consistent with our theoretical model, we predicted that the final ACE indicators would reflect a continuum of clinical relevance, ranging from a high risk of family violence (i.e. high need for intervention) to lower relevance, consistent with previously studied ACEs domains.
Challenges in defining ACEs
Since the late 1990s, the initial "ACE domains" have undergone numerous expansions across studies. Whilst this variation helped innovate and adapt indicators of ACEs to different goals, there is currently little consistency in the definition and inclusion of ACEs. The large variation of measured ACEs also means there is no agreed reference standard for developing new measures of ACEs.
Previous studies have mainly assessed the validity and relevance of ACEs based on their risk association with poorer health outcomes in adulthood. However, most studies reporting on the negative health effects of ACEs are based on cross-sectional samples of adults asked to recall experiences from childhood1. Recent birth cohort studies, however, reveal that ACEs are relatively poor predictors of negative health outcomes in adulthood relative to other socioeconomic factors2.
Global studies by the World Health Organization show that traumatic stress symptoms naturally resolve on average six years after a linked traumatic event (e.g., an ACE)3, 4.
These gaps create multiple challenges when attempting to develop new indicators of ACEs for electronic health records (EHRs).
Establishing a consistent definition
To enhance consistency in developing clinically relevant ACE indicators for different data sources, we conducted several studies4 to establish a definition of ACEs based on a set of criteria. We also developed a testable theoretical biopsychosocial model of ACEs. This model facilitates theoretically informed predictions of which ACE indicators might be more relevant than others.
Definitions and Inclusions
We defined ACE indicators as any experience within the family environment recorded in the child or the parent data source (e.g. health record) considered to be:
- Frightening, violent, traumatic or neglectful (see WHO violence definition), with potential for immediate or longer-term harm to a child's biopsychosocial development (intentionally or unintentionally) (see UK government definition);
- Caused by a single event or through repeated exposure;
- Caused by external factors and not the child themselves, such as self-harm; and
- Amenable to health or social care intervention at a family level (i.e. excluding wider factors such as socioeconomic status, community violence, school bullying etc.)1, 2, 3.
We made several adaptations to previously studied ACEs for feasible ascertainment in electronic health records (EHRs). We defined indicators as variables of grouped codes and measures. We aimed to develop ACE indicators that reflected clinically meaningful risk groups of adversity to identify families that may be eligible for targeted maternal-child care interventions in England (e.g. Supporting Families programme, or previously "targeted care pathway" of the Healthy Child Programme. See also WHO for intervention studies).
We manually grouped indicators into broader ACE domains consistent with the original study by Kaiser Permanente and CDC. Due to the lack of recordings, we collapsed all types of child abuse and neglect into child maltreatment (CM). We collapsed "imprisonment of household members" and "household challenges" into Adverse family environments. We created a separate indicator, "Social service involvement" (SSI), for social care-related codes that did not contain descriptions of CM or IPV. Due to few recordings and high intercorrelations, SSI was merged with CM in the final selection process.
Given the substantial under-recording of CM and IPV1, 2, we also added the domain “high-risk presentations of CM” (HRP-CM). HRP-CM encompassed indicators from the National Institute for Health and Care Excellence (NICE) and Royal College of General Practitioners (RGCP) that should raise clinical suspicion for CM.
Note: ACEs can be recorded in both parents’ and children’s records. ACEs are considered based on each specific child’s time from birth. Children are, therefore, considered unexposed if no relevant recording occurs during the study period, regardless of previous exposure to children within the same family. This approach mirrors changes in stress levels as the family moves through different life stages.